
 Laminitis, often referred to as “founder”, is a term that triggers fear in many horse owners. The problem can be life-threatening, and currently accounts for almost 2% of the horses referred to The Atlanta Equine Clinic for treatment. Laminitis is defined as inflammation of the laminae of the foot.
Laminitis, often referred to as “founder”, is a term that triggers fear in many horse owners. The problem can be life-threatening, and currently accounts for almost 2% of the horses referred to The Atlanta Equine Clinic for treatment. Laminitis is defined as inflammation of the laminae of the foot.
What are LAMINAE?
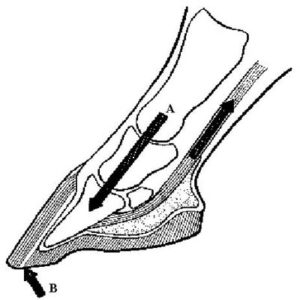
Laminae are finger-like protrusions of tissue. In the equine foot, there are 2 types of laminae: sensitive (dermal) laminae and insensitive (epidermal) laminae. These two types of laminae interdigitate with each other to form a bond that is responsible for holding the hoof wall onto the horse’s foot. It is very similar to the mechanism by which our finger nail (insensitive) is attached to our finger (sensitive). Each foot contains approximately 600 primary laminae. Each primary lamina, in turn, contains approximately 100 secondary laminae. Laminae in the horse’s foot undergo significant shear (A) and distractive (B) forces as a result of weight bearing.
How do laminae become inflamed?
There are many predisposing factors that trigger the onset of laminitis. Regardless of the original cause, however, compromised blood flow is thought to be involved in the final pathway that eventually results in laminar inflammation and pain. This becomes an important consideration when determining an appropriate course of treatment for laminitis. Predisposing factors for laminitis include:
- Grain overload. Ingestion of an excessive amount of grain can alter the bacterial balance within the cecum, which is the “fermenting” organ of the horse’s GI tract. Consequently, bacteria that produce lactic acid (such as Lactobacillis and Streptococcus spp.) tend to proliferate. The presence of increased lactic acid (and decreased pH) can lyse the cell wall of gram negative bacteria. This results in the release of endotoxins within the cecum. If absorbed into the systemic circulation, endotoxins can cause compromised blood flow of the peripheral circulatory system. Altered blood flow in the feet can trigger laminitis.
- Systemic infection and/or endotoxemia.Endotoxemia refers to the presence of endotoxins within the bloodstream. Endotoxins are absorbed into systemic circulation through compromised tissue. Various forms of colic can result in compromise of the gastrointestinal mucosa. Endometritis (such that occurs with a retained placenta) can cause compromise of the endometrium within the uterus. If bacteria (and therefore endotoxins) are present, their absorption through compromised tissue is possible. Once in the bloodstream, the presence of endotoxins can dramatically affect blood perfusion within the feet and therefore laminar integrity. Laminitis resulting from endotoxemia is usually severe.
- Obesity.Extra weight increases the shearing and distractive forces applied to the feet, thereby facilitating laminar breakdown. Hypothyroidism generally results in increased weight gain in horses, and therefore is often considered a predisposing factor to laminitis.
- Grass ingestion. This is often referred to as “grass founder”, and generally occurs in the early spring when fresh new grass is growing. Although this cause of laminitis has not been completely explained, a high content of fructans (a specific carbohydrate) within the grass has been implicated.
- Cold water ingestion. The pathophysiology is uncertain, but ingestion of excessive amounts of cold water has been associated with laminitis.
- Excessive concussion to the feet.Trauma to the feet can result in altered perfusion of the capillaries within the laminae. A condition called “foot strike hemolysis” has been described in race horses and refers to lysis of red blood cells within the feet. Vasoconstriction and coagulation often accompany excessive concussion to the feet.
- Chronic overloading of the feet.This becomes a concern in situations in which a horse has moderate to severe lameness of one or more limbs and is forced to over- bear on another. Chronic overloading can result in reduced and/or redistributed perfusion within the foot.
- Excessive amount of steroid.An excessive amount of circulating steroid may have an effect on perfusion in the equine foot. Regardless of whether it is man-made or horse-made, its presence can increase the risk for developing laminitis. Veterinarians should be aware of potential risks when administering steroid to horses, and pay careful attention to the type of steroid being used, its recommended dosage, the route of administration, and the current health status of the animal. Some conditions in the horse can result in excessive production of endogenous (horse-made) steroid, the most common of which is pituitary adenoma (Cushings Syndrome). Recently, this disease has been associated with a significant number of laminitis cases in older horses. In horses that show signs of laminitis or are at increased risk, treatment for Cushings is recommended.
- Hormonal causes. The relationship between hormones and laminitis is currently unclear. Laminitis has been observed in some mares with no apparent cause. Signs resolve quickly at the onset of estrus (heat). In other mares, development of laminitis was attributed to persistent estrus.
- Ingestion of certain substances. Some substances have been directly associated with the development of laminitis in horses. Beet tops is one example.
- Pain. Pain in the horse results in stimulation of the sympathetic nervous system and the release of catecholamines within the blood stream. Systemic catecholamines cause peripheral vasoconstriction and decreased blood flow to the foot, which in turn can result in further laminar compromise, inflammation, and more pain. Breaking the “pain cycle” is an important part of successful treatment for laminitis.
- Unknown causes.Many cases of laminitis cannot be traced to a specific cause.
Mechanical founder is a term that refers to loss of laminar integrity in the absence of initial vascular and/or metabolic compromise within the foot. Most horses experiencing mechanical founder are not lame; however, delamination and rotation of the third phalanx within the hoof capsule is apparent.
Chronic excessive tension of the deep digital flexor (DDF) tendon is implicated as the primary cause of mechanical rotation. Excessive pull of the third phalanx in a palmar direction can result in considerable distraction along the laminar interface (C). If distraction is severe enough and/or occurs for a long enough period of time, laminar separation (delamination) may ensue. Consequently, chronic thickening of the white line, sub laminar infection (“seedy toe”), and hoof wall deterioration are common findings in horses experiencing mechanical founder. Horses with broken-back distal limb axes have increased DDF tendon tension and are therefore more prone to developing mechanical founder. Treatment usually consists of corrective shoeing designed to normalize the distal limb axis, facilitate limb breakover, and alleviate DDF tendon tension.

What is “digital collapse”?
Digital collapse refers to movement of the third phalanx independently of the hoof capsule. There are 2 basic ways in which the third phalanx can collapse:
- ROTATION and
- SINKING
Rotation refers to distraction of the dorsal aspect of the third phalanx away from the dorsal hoof wall (C). Following rotation, the angle of the third phalanx differs from that of the hoof wall. Since tension of the deep digital flexor tendon plays a significant role in rotation (D), mechanically alleviating DDF tension is typically a first line treatment approach. Sinking refers to vertical displacement of the third phalanx relative to the hoof capsule. The third phalanx “slides” through the hoof capsule towards the ground. In order for this to occur, the laminar bond must break down circumferentially. Usually the dorsal aspects of the hoof wall and third phalanx remain parallel. Sinking is more a result of shear weightbearing forces (E) applied to the foot rather than DDF tendon tension and is therefore more challenging to manage.
What are clinical signs of laminitis?
The most obvious sign of laminitis is lameness. Since the horse normally bears more weight on the thoracic (front) feet relative to the pelvic (back) feet, clinical signs are typically worse in the thoracic feet. In most cases, only the thoracic feet are involved. In these cases the horse will often place the hind feet well up under the abdomen and the front feet forward with the weight on the heel of the foot. If all four feet are involved, horses will usually carry the front feet back and the back feet forward to create a very narrow base of support. Lameness is usually very apparent when turning the horse in small circles on a hard surface. Degree of lameness has been characterized by the following criteria:
Grade 1:
The horse will alternately lift the feet at rest. The horse is sound at a walk but a shortened stride is noted at the trot.
Grade 2:
Horses move willingly at a walk, but the gait is shortened. A foot can be picked up without difficulty.
Grade 3:
The horse moves very reluctantly and resists picking up a foot.
Grade 4:
The horse refuses to move but is willing to stand.
Grade 5:
The horse is unable to stand.
What are the PHASES of laminitis?Heat is often present over the coronet band and/or hoof wall, although this finding is extremely variable. There is often an increased digital pulse and heart rate. Horses may be anxious in more severe cases.

There are 4 phases of laminitis: the developmental phase, the acute phase, the subacute phase, and the chronic phase.
The developmental phase is initiated when the horse experiences or comes in contact with one of the predisposing factors. A horse that just finished a large bag of grain but is not yet exhibiting lameness would be considered to be in the developmental phase. This phase ends at the onset of visible lameness.
The acute phase begins at the first appearance of lameness and lasts until one of two things happen: 1) the passing of 72 hours without physical or radiographic evidence of delamination (or the breakdown of the laminar interface) or 2) digital collapse (rotation and/or sinking). This phase can last anywhere from 24 hours (in severe cases) to 72 hours.
The subacute phase of laminitis begins after clinical signs persist for longer than 72 hours and there is no clinical or radiographic evidence of digital collapse. The duration of this phase is highly variable. During the subacute phase, the foot attempts to recover from damage incurred during previous phases. This can therefore be considered the “healing phase” of laminitis. Some horses will not experience the subacute phase and move directly into the chronic phase from the acute phase. Others may remain in the subacute phase for an extended period of time.
Horses enter the chronic phase of laminitis when they experience mechanical collapse of the third phalanx, regardless of when it occurs. This phase may last for an extended period (months, years, life), and is characterized by persistent lameness and/or a diverging growth pattern within the foot (multiple lines or “rings” on the hoof capsule).
What are the goals of treatment?
In some cases, horses have been exposed to one or more of the predisposing factors of laminitis but have not begun to exhibits clinical signs. During the developmental phase, therefore, the goal of treatment is prevention. Although the horse may never develop laminitis, aggressive (preventative) treatment is important to counteract the effects of biomechanical and/or metabolic derangement(s) before they occur. Once abnormalities exist, they are more difficult to treat.
The primary goal of therapy during the acute phase of laminitis is to normalize the laminar environment and prevent further deterioration of the laminar bond. This is attempted by decreasing pain, reducing inflammation, and minimizing mechanical stress to the third phalanx while enhancing blood flow to the foot. Undoubtedly, horses that do not demonstrate laminar separation and digital collapse within 72 hours are more likely to experience full recovery.
In the subacute phase of laminitis, the goal of therapy is designed to reestablish normal laminar integrity and strength, thus avoiding progression into the chronic phase. The horse’s response to corrective trimming/shoeing usually dictates the duration of time that they spend in this phase.
Rehabilitation is the main focus of treatment during the chronic phase. Some horses never fully recover from this phase and must be managed their entire remaining lives. As might be expected, collapse of the third phalanx changes the operative pathologies and mechanical properties within the foot considerably. Consequently, mechanical support of the foot, vascular integrity of the laminae, general metabolism, growth abnormalities in the hoof wall, and foot pain are important issues in regard to appropriate therapy during this phase.
What does treatment for laminitis involve?
In order to treat laminitis effectively, we must:
- Eliminate all predisposing factors. Avoiding the ingestion of grain and/or large amounts of fresh grass, reestablishing normal foot angle, losing weight, minimizing exercise, and addressing metabolic derangement(s) are all ways of discouraging the development and/or the progression of laminitis.
- Mechanically support the third phalanx. Since we can no longer rely on the laminar bond to support the weight of the limb, we must eliminate the shearing forces between the third phalanx and the hoof wall. This is typically accomplished by trimming the hoof wall back far enough to allow weightbearing on the sole and frog (F, G).
- Minimize tension on the deep digital flexor (DDF) tendon. Initially this is accomplished by elevating the heel relative to the toe, thereby decreasing the distance between the origin and insertion of the DDF tendon. Use of a heel wedge (H) reduces DDF tendon tension and therefore distractive forces across the laminar interface.However, change in angle of the third phalanx may result in increased shearing forces. Therefore, heel wedging may be detrimental in cases in which “sinking” is evident.
Once laminar integrity is reestablished, returning the foot to a normal angle may be possible. Of course, this is done over a period of time. In severe cases, surgical intervention in the form of distal accessory (check) desmotomy or DDF tenotomy may be necessary to effectively relieve DDF flexor tension.
- Reduce pain. Since pain can adversely affect blood flow to the feet (via the release of catecholamines), maximizing comfort is an essential part of reestablishing laminar integrity and initiating healing. Local anesthetics (foot blocks), pain relievers, and anti-inflammatory medications are effective ways of reducing pain.
- Reduce inflammation within the foot. The hallmark of inflammation is vasulitis, or inflammation of the blood vessels. When inflamed, the vessel walls become more permeable. Increased permeability within the vessel walls results in the leakage of proteinaceous fluid from the vessels into the surrounding tissues. This extravascular fluid is called edema. The rigidity of the hoof wall wall coupled with the formation of edema can result in a compartment syndrome, whereby elevated intralaminar pressure (caused by the presence of edema) further limits vascular perfusion to the foot.Phenylbutazone is an anti-inflammatory medication frequently used for laminitis. The efficacy of “bute” can be partially attributed to its vasodilating effects, which results in improved perfusion within the foot.
- Improve blood flow to the foot. Phenylbutazone, Aspirin, Isoxuprine, nitroglycerin, and Acepromazine are medications frequently used in an attempt to enhance vascular perfusion within the foot.
