
 Distal tarsitis, often referred to as “bone spavin”, is the most common cause of clinical lameness associated with the tarsus (or “hock”) in horses. Distal tarsitis is an osteoarthritis and periostitis of the distal intertarsal, tarsometatarsal, and occasionally the proximal intertarsal joints.
Distal tarsitis, often referred to as “bone spavin”, is the most common cause of clinical lameness associated with the tarsus (or “hock”) in horses. Distal tarsitis is an osteoarthritis and periostitis of the distal intertarsal, tarsometatarsal, and occasionally the proximal intertarsal joints.
How does distal tarsitis arise?What are the distal tarsal joints?
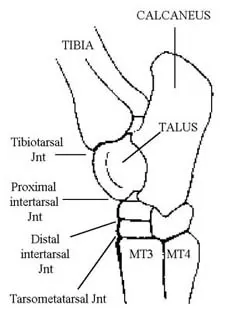
The tarsus, or “hock”, is very similar in structure to the human heel. The tarsus consists of 4 joints: the tibiotarsal joint, the proximal intertarsal joint, the distal intertarsal joint, and the tarsometatarsal joint. During movement, the tibiotarsal joint performs approximately 98% of the motion of the tarsus. The proximal intertarsal joint, just below the tibiotarsal joint, performs approximately 2% of the motion. The lowest 2 joints, the distal intertarsal and tarsometatarsal joints, move very little. In fact, if the horse did not have these joints (i.e. if there was solid bone across the distal tarsus) we would not be able to detect any unsoundness or alteration in gait.
Although the distal tarsal joints are not essential to normal locomotion of the horse, they are prone to instability. Chronic joint instability results in the development of joint inflammation (i.e. arthritis). Repeated compression and rotation of the tarsal bones and excessive tension on the attachment of the major dorsal ligaments have been implicated as causes of distal tarsitis. Factors which can affect the development of distal tarsitis include the horse’s age, weight, breed, job description, frequency of work, intensity of work, and conformation.
Following are conformational abnormalities which may increase the horse’s chances of developing distal tarsitis:
- Straight pelvic limbs
- Sickle hocks
- Cow hocks
What are the clinical signs?
Horses with distal tarsitis usually exhibit a gradual onset of pelvic limb lameness. Lameness is most apparent during the trot and may be characterized by a hypermetric “stabby” pelvic limb flight pattern. Horses will commonly pull the pelvic limbs underneath their body and “stab” them to the outside as the foot strikes the ground surface. Although lameness is frequently bilateral, horse’s will favor the more affected limb during exercise. A “hip hike” (pelvic excursion) is typically apparent, particularly when the horse is trotting with the affected limb to the inside of a circle. Lameness may worsen following a period of rest. Affected horses usually exhibit stiffness when first starting to exercise but can often “work out of it”. In chronic cases, firm enlargement on the inside of the hock may become visible; the swelling represents excessive proliferation of bone associated with the distal tarsal joints. Horses with moderate to severe tarsitis will usually exhibit a positive Churchill’s Hock Test, a procedure which is performed during the passive lameness evaluation. A positive response to this test is manifested by pelvic limb abduction. Pelvic limb flexion (“spavin testing”) during active lameness evaluation is an accurate and widely used detector of distal tarsitis. A positive response results in increased lameness and hypermetria following 60-90 seconds of pelvic limb flexion prior to trotting.
It is very common for horses to exhibit secondary symptoms as a consequence of favoring one or both pelvic limbs over an extended period of time. Common compensatory problems include:
- Thoracolumbar ebaxial (back) soreness due to an asymmetric pelvic limb gait
- Proximolateral thoracic limb suspensory desmitis as a result of chronic overloading of the thoracic limbs
- Greater Trochanteric Bursitis (“whorlbone”) as a result of the abnormal pelvic limb gait
- Increased wear on the outside of the pelvic foot or shoe– in an attempt to relieve hock pain
Since these abnormalities are often secondary to distal tarsitis, successful treatment of the tarsitis alone frequently results in resolution of these problems. In our opinion, horses that exhibit one or more of the above mentioned clinical signs should be evaluated for the presence of distal tarsitis as a potential primary cause.
How is distal tarsitis diagnosed?
Distal tarsitis is a clinical diagnosis. In other words, demonstration of pain in distal tarsal joints is diagnostic. Pain is demonstrated upon clinical examination, lameness characteristics, response to Churchill’s Hock Test and hock flexion, and response to intra-articular anesthesia. Radiographs are frequently used to assess the presence and severity of distal tarsitis. It is important to note, however, that joint inflammation (arthritis) is invisible on a radiograph (which provides only structural information). Since the tarsus is a low-motion area, radiographic changes and the presence of distal tarsitis do not always correlate. Nuclear scintigraphy (bone scanning) may be a more accurate assessor of the presence of distal tarsal inflammation since it provides functional information (i.e. measures bloodflow). In our experience, this diagnostic modality has proved to be very useful in the identification of distal tarsitis.
How is distal tarsitis treated?
Two basic forms of treatment exist for distal tarsitis. The first involves the reduction and possibly the elimination of inflammation within the distal tarsal joints. This is achieved by the use of systemic and/or intra-articular anti-inflammatory therapy. Reduction of inflammation (arthritis) results in improved comfort. Intra-articular therapy usually involves the use of steroids, which are extremely effective at reducing local inflammation and pain. This approach also involves an attempt to maintain normal synovial integrity within the distal tarsal joints. Systemic medications such as Adequan®, Legend®, Cosequin®, etc. are designed to improve synovial function and general joint comfort in the horse. Clinicians at The Atlanta Equine Clinic also use intra-articular hyaluronan therapy (in combination with steroids) to enhance the effect of the treatment locally.
The other form of distal tarsal therapy involves fusion of the distal intertarsal and tarsometatarsal joints. This can be accomplished surgically or by the use of a chemical agent which is infused into the distal tarsal joints. Since these joints have almost no motion, their fusion results in minimal alteration in the horse’s gait. By eliminating the joints, however, instability and therefore inflammation and pain are also eliminated. This approach is generally reserved for those horses that have proved to be refractory to anti-inflammatory treatment and have advanced osseous changes associated with the distal tarsal joints. If you would like to learn more about distal tarsal fusion, please ask one of our staff. We will be glad to discuss this topic in more detail.