
Navicular inflammation, often referred to as “Navicular Disease” or “Podotrochleosis”, is one of the most common causes of intermittent, often-shifting, thoracic limb lameness in horses between 4 and 15 years of age. Although the pelvic limbs may be affected, for all intents and purposes it is a disease of the thoracic limbs.
Where is the “Navicular Bone”?
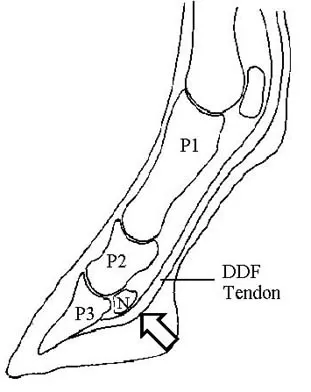
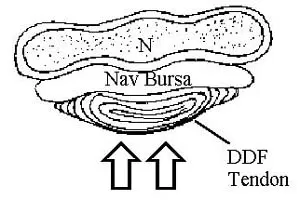
The navicular bone resides palmar to the coffin joint in the back 1/3 of the foot. It serves as a fulcrum for the deep digital flexor (DDF) tendon as this structure passes around the back of the foot to attach on the third phalanx (P3 or “coffin bone”). The navicular bone consists of a hard cortical exterior and a soft cancellous interior (medulla or marrow). The soft marrow interior allows the navicular bone to compress when under pressure. The navicular bursa is a synovial “sac” between the navicular bone and DDF tendon and serves to lubricate the tendon as it slides over the back of the navicular bone.
How Does Navicular Inflammation Arise?
Simply, inflammation in the palmar foot or navicular area develops as a result of excessive tension of the deep digital flexor (DDF) tendon. Since the DDF tendon uses the navicular bone as a fulcrum, increased DDF tension results in increased pressure across the navicular bone. In the normal situation, the navicular bone responds by compressing. However, if the pressure is persistent and/or severe, the navicular bone will begin to remodel in an attempt to adapt to the biomechanical stimulus. During remodeling, osteoblasts (hard bone cells) are laid down along the palmar surface of the marrow cavity. This results in a higher hard bone:soft bone ratio which increases the bone’s stiffness and decreases its compressibility. If the pressure is of low intensity and/or of limited duration, navicular bone remodeling may successfully absorb, diffuse, and redistribute the load. In this situation, horses will remain asymptomatic. However, if the pressure is of high intensity and/or persistent, inflammation (and pain) may ensue.
Why Does Navicular Inflammation Occur?
Other contributors to navicular inflammation include navicular bursitis (inflammation of the navicular bursa) and venous congestion/hypertension within the navicular bone. Both may also occur as a result of excessive DDF tension.
Horses can have excessive DDF tension for a number of reasons. The horse’s breed, size, type of work, frequency of work, intensity of work, conformation, etc. can all play a role in the development of navicular inflammation. Since it is our goal to keep your horse performing at its intended level, we will only discuss factors which are treatable. Many are related to conformation. The most common are:
- Broken-back Distal Limb Axes. This conformation results in an increased distance between the DDF tendon’s origin in the DDF muscle along the back of the radius and its insertion on the palmar aspect of the third phalanx. Since this tendon stretches very little, increasing its traveling distance increases its tension. Increased DDF tension results in increased pressure across its fulcrum (the navicular bone).
- Low Heels/Long Toes. This conformation delays the breakover of the limb. The more delayed the breakover, the greater the DDF tension prior to advancing the limb. The more DDF tension, the more pressure on the navicular bone.
- Underslung Heels. Due to the anatomy of the fetlock joint, a horse’s center of gravity is actually behind (palmar to) where the foot rests on the ground surface. Weightbearing force is therefore greatest on the palmar aspect of the foot closest to the limb’s center of gravity. The greater the distance between the foot and the center of gravity, the greater the weightbearing force on the back of the foot. Underslung heels are farther from the center of gravity of the limb, and are therefore subject to greater weightbearing or concussive forces. Frequently, the navicular bone lies just above the point where the heel meets the ground and the force is the greatest. Underslung heels, therefore, result in increased concussive pressure on the navicular bone.
- Sheared Heels. This refers to unbalanced heels; i.e. where the heels are at different levels relative to the ground surface. Since the navicular bone lies across the back of the foot, it experiences differences in forces from one side of the foot to the other. This abnormality, therefore, may not only increase overall navicular pressure, but result in differences in pressure from one side to the other.
What are the clinical signs?
Affected horses often have a history of intermittent thoracic limb lameness that improves with rest. Although both forefeet are usually involved, the lameness is only observed in the more affected limb. It is not until perineural anesthesia is used to anesthetize the more severe foot that a contralateral lameness is manifested. Subsequent perineural anesthesia of the contralateral limb often produces a sound horse. Following are some common clinical and lameness characteristics of horses with navicular inflammation:
- High and/or contracted heels on the affect foot (often thrush is present).
- Grade 2-3/5 thoracic limb lameness.
- Consistent pointing with the affected limb.
- May stand in the stall with the toes stuck down in the bedding.
- Chronic bruising of the sole and/or toe.
- Worse when trotting with the affected limb on the inside of a circle.
- Horse tends to land on the toe during movement.
- Sensitivity to pressure (hoof testers) over the frog of the affected limb.
- 100% soundness is achieved with palmar digital (PD) perineural anesthesia of the limb.
How is Navicular Inflammation Diagnosed?
Navicular Inflammation is a clinical diagnosis. In other words, demonstration of pain in the palmar aspect of the foot is diagnostic of navicular inflammation. Pain is demonstrated upon clinical examination, hoof testing of the frog, and response to PD perineural anesthesia. Radiographs are frequently used to assess navicular inflammation. It is important to note, however, that inflammation is invisible on a radiograph. Since this is a relatively low-motion area, radiographic changes and the presence of navicular inflammation don’t correlate very well. Therefore, we must rely on our clinical findings to determine the presence of navicular inflammation and pain.
How is Navicular Inflammation Treated?
- CORRECTIVE SHOEING
- Maintain straight distal limb axes (to decrease DDF tendon tension)
- Trim, broaden, and rocker the toes (to quicken breakover and decrease DDF tendon tension during movement)
- Apply full (egg) bar shoes (to stabilize the heels relative to one another and prevent shearing)
- Extend the shoe palmarly (to move the point of weightbearing closer to the limb’s center of gravity)
- MEDICATION DESIGNED TO ENHANCE PERIPHERAL BLOODFLOW
- Aspirin: Prevents platelet aggregation and therefore “thins” the blood
- Isoxuprine: A vasodilator (increases the diameter of the vessels)
- Phenylbutazone: A vasodilator
- SYSTEMIC ANTI-INFLAMMATORY MEDICATION
- Phenylbutazone: Functions as both a vasodilator and anti-inflammatory
- Previcox: A long-term anti-inflammatory
- SYSTEMIC ARTHROTHERAPY
- Adequan, Legend, Cosequin, Flex-Free, etc. can help normalize the synovial environment within the navicular bursa and reduce inflammation/pain.
- LOCAL ARTHROTHERAPY
- In cases of chronic moderate to severe navicular inflammation, we often elect to perform intrasynovial injection. This may involve direct navicular bursa injection and/or indirect delivery of medication to the bursa via the distal ingterphalangeal (or coffin) joint.
- TILDREN
- This product has proven to be very effective at alleviating inflammation and clinical signs associated with navicular inflammation in our hands.
- EXTRACORPOREAL SHOCK WAVE THERAPY (ESWT)
- Shock wave therapy has shown to be an effective treatment modality for navicular inflammation, especially if concurrent deep digital flexor tendon (DDFT) pathology exists.
- PERMANENT ANESTHESIA OR PD NEURECTOMY
- This is the ultimate “pull the wool over your eyes” technique. Eliminating the horse’s ability to feel pain certainly improves soundness; however, it also greatly increases the risk of the horse sustaining injury to the numbed portion of the foot. Therefore, this approach should only be considered as a last resort.
In summary, navicular inflammation appears to be a disorder triggered by an excessive bone remodeling response. Bone remodeling occurs as a result of excessive pressure across the navicular bone by the DDF tendon. Excessive DDF tendon tension may occur due to faulty conformation that is acquired or inherited. Navicular inflammation can be successfully managed via early recognition and correction of the predisposing factors as well as a proper therapeutic plan.