
Charles, a 14 year old Warmblood gelding, was seen for an acute right forelimb lameness noted 2 days prior. On presentation, there was no palpable heat or swelling in the limb and there was mildly increased digital pulse quality. He was not sensitive with hoof tester pressure. Manipulation of the limb revealed decreased range of motion of his right front fetlock. He demonstrated grade 3/5 right forelimb lameness when trotted in hand on soft footing. Distal limb flexion concentrated on the fetlock and below elicited a more severe lameness (grade 4/5) in his right forelimb. (Grade 0/5 = sound, Grade 5/5 = unable to bear weight) A palmar digital nerve block (“heel block”) improved the lameness significantly (85 – 90%). An intermittent off step was noted on the right front, especially when circling to the left at the trot. Additionally, he continued to show resentment and increased lameness after distal limb (fetlock) flexion. Following a sterile scrub, an intra-articular block of the right front fetlock joint was performed next. The joint fluid seemed excessive and of poor quality (watery). This block improved the lameness further – he was sound in both directions at the trot and no longer resented manipulation or flexion of his fetlock. Radiographs (“x-rays”) revealed osteoproliferation (“lipping”) of the dorso-proximal aspect of P2 (long pastern bone) and osteoproliferation at the insertion of the distal sesamoidean ligaments along the palmar aspect (or back) of the pastern. There appeared to be decreased joint space of the right front fetlock joint and osteoproliferation (“lipping”) at medial (inside of the leg) aspect of joint with irregular bone margins noted at the joint capsule attachment. A magnetic resonance imaging (MRI) exam was recommended at this time to further evaluate the bones and fully evaluate the soft tissue structures of the distal limb.
The MRI images combined with the radiographic findings gave us a complete picture of the problem within Charles’ right front limb. This allowed us to formulate a plan of targeted therapy as well as a prognosis for soundness.
[ezcol_1half] [/ezcol_1half][ezcol_1half_end]
[/ezcol_1half][ezcol_1half_end] [/ezcol_1half_end]
[/ezcol_1half_end]
The MRI images were obtained with Charles standing, mildly sedated in a Hallmarq 0.3T MRI magnet. He was not a candidate for an MRI which would require general anesthesia, as his owner did not want to incur the potential hazards and risks associated with general anesthesia; nor did she want to potentially cause him further injury when he recovered from general anesthesia. Horses often times scramble when they recover from anesthesia and could cause further damage to already injured area.
[ezcol_1third]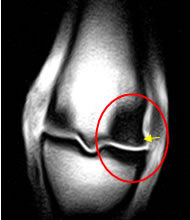
T1W3DFRO
T2*WFRO

STIR FSE FRO
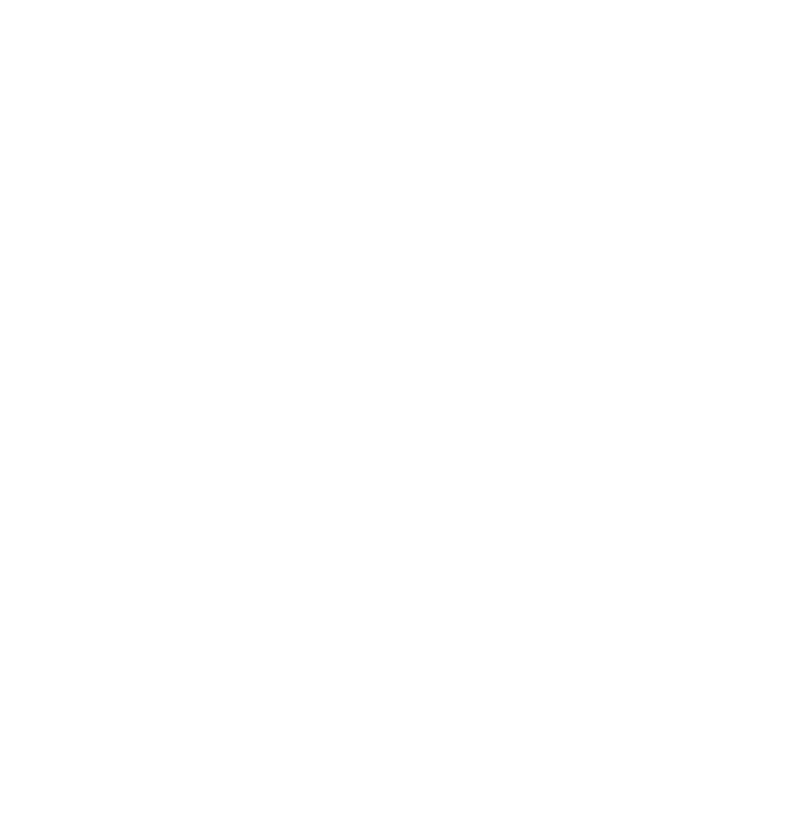
MRI frontal images of the right front fetlock showing the large area of sclerosis (red circle) and full thickness cartilage and subchondral bone injury (yellow arrow) to the medial condyle of the cannon bone.
[ezcol_1half]
T2FSE SAG

STIR FSE SAG
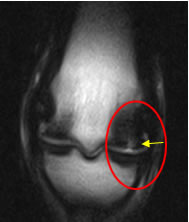
MRI sagittal images of the right front fetlock showing sclerosis (arrowheads) and cartilage defect (white circle) of the medial condyle.
The MRI study revealed numerous mild changes of the pastern and foot including the following: mild synovitis (inflammation) in the distal interphalangeal (coffin) joint and proximal interphalangeal (pastern) joint; enthesiophyte formation and sclerosis at the insertion of the lateral collateral ligament of the distal interphalangeal joint (indicating joint capsule stretching and strain); mild fraying and thinning of the axial margin of the lateral collateral ligament of the distal interphalangeal joint at the level of the insertion of the distal phalanx (sprain/injury at the coffin joint). Irregular bone margins on the palmar aspect of the first phalanx at the insertion of the oblique sesamoidean ligaments (chronic bone changes due to micro tears along the area where the sesamoidean ligaments attach to the bone).
MRI of the right front fetlock revealed the most significant findings. A focal subchondral bone defect was identified in the distal medial aspect (inside portion of the end) of the third metacarpal bone (cannon bone). This defect was located immediately dorsal to the transverse ridge. It measured 4 mm in diameter (medial to lateral) and was surrounded by a large area of sclerosis (bone reaction). A more extensive area of flattening (15mm) was also identified in the dorsal to palmar dimension (front to back) associated with this lesion. There was focal fluid in the trabecular bone immediately proximal to the subchondral bone defect. This finding is most consistent with focal osteonecrosis (inflammation and weakening of the bone). Fluid in the fetlock joint can be identified extending into the subchondral bone defect indicating a full thickness articular cartilage defect. There is additional mild to moderate sclerosis in the distal lateral aspect of the third metacarpal bone and proximal phalanx (medial and lateral aspects). This indicates the bones of the fetlock joint are reacting to abnormal forces of excessive concussion and wear and tear.
Going back and reviewing the radiographs did show a very faint area of lucency (lack of bone density) on the lateral aspect of the cannon bone at the fetlock joint. Without the confirmation by the MRI, it would have been difficult to say this lucency was of clinical significance. The bone and soft tissue detail gathered by the MRI made the injured areas very obvious. In fact, the MRI also detailed numerous other areas involving the coffin bone and pastern.
On the day following his MRI, we repeated the right front fetlock joint block to see what percentage of the lameness was a result of the injuries noted in the fetlock, and what percentage may be from his other abnormalities. Charles was completely sound after the fetlock joint block. The MRI findings in the right front fetlock were consistent with severe and most likely permanent structural injury to the third metacarpal bone (cannon bone) and the fetlock joint and likely the cause of Charles’ current lameness. Such an injury requires strict management for the next 6-9 months before knowing how this will affect his ability to be a riding horse long term.
These findings and a guarded (possibly grave) prognosis for return to soundness as a competitive horse were discussed with the owner. Surgical arthroscopic evaluation, debridement and treatment with therapies were recommended. Surgical exploration was declined by the owner. The owner did elect to have a series of intra-articular Interleukin-1 Receptor Antagonist Protein (IRAP) treatments to the right front fetlock joint combined with rest and controlled rehabilitation. IRAP is made from the horse’s own blood and acts a very potent anti-inflammatory which would allow the structures to heal with minimal scarring.
Although Charles’ owner was disappointed his competitive career had come to a close, she was happy she found out his reason for his lameness. She was also happy not to have continued to medicate him and keep him in full training for any longer at her expense and his discomfort. At 3 months follow up, Charles was sound at the walk and with limited trot. He has essentially been retired to a pleasure trail horse.