
 Canajoharie is a 9 YO THB gelding. He was displaying signs of abdominal discomfort including pawing, looking at the flanks, and attempting to lie down. Dr. Bueno, our board certified surgeon, was on call for the evening and was immediately dispatched to the barn for an evaluation. The owners had given a 1,000 lbs dose of flunixin meglumine (“Banamine”) orally approximately 1.5 hours before Dr. Bueno’s examination. The examination revealed a mildly elevated heart rate (48 bpm), slightly distended large colon on palpation per rectum, and signs of mild-moderate abdominal pain. The horse was treated medically with pain relievers, or analgesics, (xylazine and butorphanol), and oral mineral oil and electrolytes via a nasogastric (“stomach”) tube. Dr. Bueno advised the owners that their horse may need further treatment at a facility equipped to perform colic surgery. The owners were initially hesitant to do so.
Canajoharie is a 9 YO THB gelding. He was displaying signs of abdominal discomfort including pawing, looking at the flanks, and attempting to lie down. Dr. Bueno, our board certified surgeon, was on call for the evening and was immediately dispatched to the barn for an evaluation. The owners had given a 1,000 lbs dose of flunixin meglumine (“Banamine”) orally approximately 1.5 hours before Dr. Bueno’s examination. The examination revealed a mildly elevated heart rate (48 bpm), slightly distended large colon on palpation per rectum, and signs of mild-moderate abdominal pain. The horse was treated medically with pain relievers, or analgesics, (xylazine and butorphanol), and oral mineral oil and electrolytes via a nasogastric (“stomach”) tube. Dr. Bueno advised the owners that their horse may need further treatment at a facility equipped to perform colic surgery. The owners were initially hesitant to do so.
Despite initial medical therapy Canajoharie continued to show signs of abdominal pain. The owners had now decided to transport him to the hospital at SSEC for further evaluation and treatment. Treatment at SSEC included a full colic work (ultrasound, belly tap, blood work), IV fluid therapy and additional analgesics for pain. Discussions with the owners on the fact that despite this more aggressive medical therapy he continued to show signs of abdominal pain; the decision was made to perform an exploratory laparotomy (colic surgery).
Ideally, colic surgery should be performed as soon as medical therapy has been shown not to relieve the horse’s pain and discomfort. Waiting too long can cause further bowel deterioration and also necessitate much more supportive care which translates into much more expense for the owner.
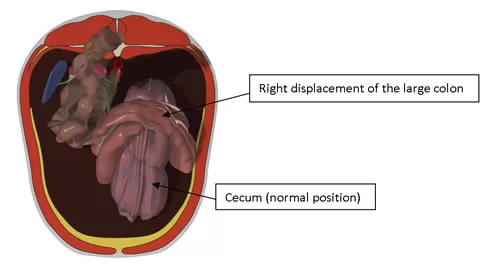
The colic surgical team was called in and within 45 minutes Canajoharie was prepped and ready for surgery. Colic surgery revealed a right dorsal displacement of the large colon with a right dorsal colon impaction. (See Fig 1.) The impaction was corrected via a pelvic flexure enterotomy (opening of the bowel to remove and flush out the contents) followed by correct repositioning of the large colon within the abdominal cavity.
The incision into the bowel was sutured closed as was the deep abdominal layer (the linea alba) and the skin. Recovery from anesthesia was uneventful. Postoperatively, Canajoharie was treated with IV fluids, broad spectrum antibiotics, NSAID (“Banamine”), and a gradual return to feeding. Canajoharie did well and was discharged 6 days later with instruction to be stall rested and hand walked to 30 days, followed by small paddock turn out for another 30 days providing that the abdominal incision has healed well, and to gradually return to work by 90 days.
Large colon displacements in horses are usually surgically correctable diseases with an excellent prognosis for return to activity. However, recurrence has been reported (8-12%). One of potential causes of large colon displacement is that the large colon is fairly mobile because of the lack of attachments to the body wall. Another potential cause is that the motility pattern initiated at the pelvic flexure could result in displacements or torsion. Moreover, diets that are rich in carbohydrates (grain) could lead to excessive fermentation and gas production leading to distention of the large colon and subsequent displacement.
Canajoharie has done extremely well and is on his way to a return to his normal lifestyle of lessons and riding! Consistent exercise with a diet full of good roughage will be important for a healthy life for this lucky horse.

“Canajoharie” after Colic Surgery at SSEC